
Photo by Rohit Pansare / Community Health Workers
Strengthening Primary Care in an Underserved, Difficult to Access Terrain.
It is true that people don’t get health care that they deserve as a right in many parts of our country- India. And much of Chhattisgarh including rural Bilaspur epitomises that. And to make health care accessible to people, hospitals are important but not enough. Even the presence of the best hospitals in significant numbers cant ensure good health of the people. People need good quality first contact care at the village level. Plus they need sound counsel to make decisions about seeking health care for bigger problems. Third, cure of treatment may be possible, but preventive programmes necessarily have to be village and family based- no institutions can ensure that. People have to be mobilised together to take decisions for themselves at a group level in order to attempt preventive strategies. Effective village level health care programmes also help the hospitals being inundated with problems that could have been solved at the village level. And finally, the village based health services are clearly cheaper and can be as effective, if not more than hospital based health care.

JSS cluster map
We started the community health programme or Village Health Programme, as we call it here, in a cluster of 8 villages. We are now running this programme in 70 tribal villages in four clusters in the Kota and Lormi blocks of Bilaspur district. These villages are located in forests or at the forest-fringe, and many of them lack access to all weather roads.
Community Health Programme
The community health programme at JSS is structured in 3 tiers. It has the village health workers at the base, chosen by the village community from among them, and trained and supported by JSS. At the second tier are sub-centres that support clusters of up to 20 villages each which are manned by a team of 3 senior health workers, who again have been trained by JSS in clinical and community health skills. These in turn are supported by the referral centre at Ganiyari at the third tier.
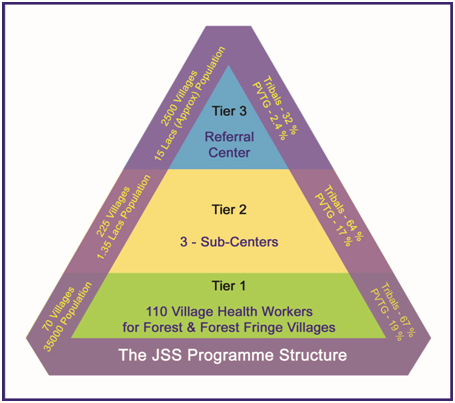
While the referral centre supports the huge unmet need for effective and low cost care for the serious and significantly complex problems that poor rural communities suffer in disproportionately large numbers, it is the village based health programme that allows us to constantly find solutions for unsolved primary health care problems. It is this programme that learns about the problems that people face, as well as doing real observational research while working.
Team
As in October 2015, the JSS programme has 110 village health workers in 54 forest and forest fringe villages in rural Bilaspur along with 93 Phulwari (crèches for under 3 year old kids) workers supported by 9 senior health workers and three Auxiliary nurse midwives(ANM). Except 4, all of them are women.

ANC clinic at Bamhani
Besides these, the supporting team includes field coordinators who support the various programmes such as maternal health including the antenatal and postnatal care, tuberculosis care, falciparum Malaria control, child health and nutrition especially under 3 age group child nutrition, use of appropriate technology in primary health, water borne diseases control and chronic diseases care. These 8 people also share responsibilities for training of health workers at the village and the sub-centres too. These frontline people are supported by two managers in each sub-centre, a total of 6, who supervise, liaise and facilitate multiple activities that go on at the sub-centres.
Scope of Work
The combined scope of work done by this team includes providing first contact health care for common and important health problems, organising referrals for those problems that they can’t manage, education of the communities such as self- help groups, parents’ groups, adolescent girls and boys, support patient support groups such as those for epilepsy and sickle cell disease, organise and run programmes for antenatal care, tuberculosis, falciparum malaria and non -communicable diseases. The sub- centre weekly clinics where a physician led team visits from the referral centre are important but continuing care for illnesses and promotive and preventive care is exclusively looked after by this team. Special curative and preventive programmes in animal health and organic agriculture for better food availability are also there. Community based monitoring of public programmes in health, public distribution systems, Panchayati Raj and of education programmes are also important activities. Innovative methods of data collection, surveillance and communication through interactive voice recording systems and use of cell phones are recent inputs that have allowed us to remain a live interactive community. Careful documentation through electronic database systems allows us to run monitored analysis of our work.
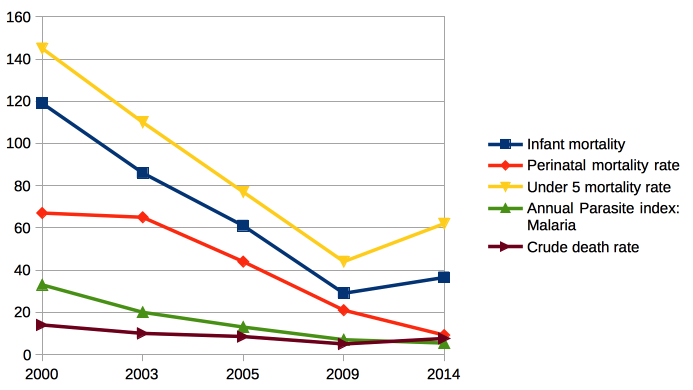
Impact & Learnings
These 15 years of work have allowed us to improve the quality of lives of people in the area, though there is a lot more to be done for one to get a feeling of contentment, and we would like to describe this as a work in progress. If one measures it in survival and nutritional anthropometric assessments or in indebtedness prevented, there are some significant gains.
Equally important have been our learnings, many of which have messages for the larger discourse in public health for the disadvantaged.
Finally, we see the need to maintain and improve this absolutely amazing interface and platform to serve, observe and learn how inequities in health of the marginalised rural poor be addressed.